

Abstract
Background
The survival of patients with multiple myeloma (MM) has improved significantly over the past two decades with the introduction of novel treatment agents. However, MM is still largely considered an incurable malignancy with a relapsing-remitting course. A follow-up of at least 10 years from active disease is required to determine whether a plateau in progression-free survival has been attained. Prior literature has used 10 years as a cutoff for "long-term survivorship". In this study, we have assessed the biological disease characteristics and outcomes of long-term survivors with MM (≥10 years from active disease).
Methods
All patients with active MM evaluated at the Mayo Clinic, Rochester between January 1, 1999 and July 1, 2008 were included in the study after approval of the Institutional Review Board. Patients with smoldering multiple myeloma were excluded. The overall survival (OS) was calculated from the time of symptomatic disease requiring treatment. Patients were then divided into two cohorts: (1) long-term survivors, which included patients who had an overall survival of at least 10 years; and (2) short-term survivors, which included patients who had an overall survival of less than 5 years from the diagnosis of active MM. The baseline characteristics between these two groups were compared using Wilcoxon, chi-square, and Fisher's exact test as applicable. All time-to-event analyses were performed using the Kaplan-Meier method and the survival curves were compared using Log-Rank test.
Results
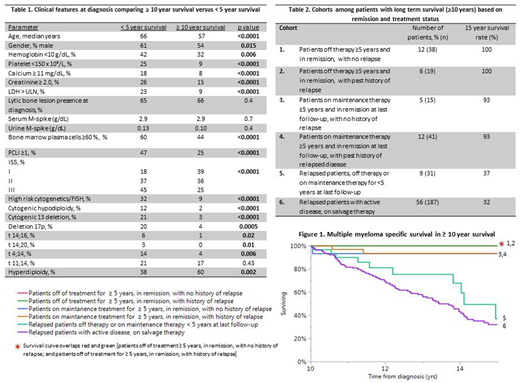
During the time frame of the study, 2,125 patients were identified who fulfilled the diagnostic criteria for active MM. The median follow-up for the entire cohort was 12.6 years (95% CI: 12.5-13.4).The median OS for the entire cohort was 4.4 years (95% CI: 4.2-4.7 years). Three-hundred and ninety nine (18.7%) patients survived at least 10 years whereas 872 patients (41%) survived less than 5 years from the date of initial diagnosis. The median OS was 14.1 years for the long-term survivors (95% CI: 13.9-14.6 years) and 2.1 years for the short-term survivors (95% CI: 1.8-2.2 years). The clinical features at diagnosis comparing long-term survivors and short-term survivors are shown in Table 1. Among long-term survivors (n=399), based on the available data regarding remission and ongoing treatment status, 331 patients were categorized into 6 cohorts (Table 2). The MM specific survival data of these 6 cohorts is depicted in Table 2.Figure 1 shows survival outcomes from the 10-year landmark. Of the 6 cohorts, 38 patients in Cohort 1 and 19 patients in Cohort 2 (total 57; 17% of long term survivors, ~3% of the entire cohort ) have been off therapy for at least 5 years and remain in remission, representing a distinct group of patients with 100% 15-year survival.
Conclusion
In our large database with prolonged follow-up, long-term survivors appear to have distinct baseline characteristics, but also constitute a heterogenous group of patients with disparate outcomes. A small subset (17% of long-term survivors) was identified that may represent patients closest to being considered as 'operationally cured'.
Lacy:Celgene: Research Funding. Dispenzieri:Celgene, Takeda, Prothena, Jannsen, Pfizer, Alnylam, GSK: Research Funding. Gertz:Teva: Consultancy; spectrum: Consultancy, Honoraria; Medscape: Consultancy; Physicians Education Resource: Consultancy; Amgen: Consultancy; Apellis: Consultancy; Alnylam: Honoraria; Abbvie: Consultancy; janssen: Consultancy; celgene: Consultancy; Prothena: Honoraria; annexon: Consultancy; Ionis: Honoraria; Research to Practice: Consultancy. Dingli:Alexion Pharmaceuticals, Inc.: Other: Participates in the International PNH Registry (for Mayo Clinic, Rochester) for Alexion Pharmaceuticals, Inc.; Millennium Takeda: Research Funding; Alexion Pharmaceuticals, Inc.: Other: Participates in the International PNH Registry (for Mayo Clinic, Rochester) for Alexion Pharmaceuticals, Inc.; Millennium Takeda: Research Funding. Kumar:KITE: Membership on an entity's Board of Directors or advisory committees, Research Funding; Oncopeptides: Membership on an entity's Board of Directors or advisory committees; Merck: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Research Funding; KITE: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees; AbbVie: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Research Funding. Kapoor:Celgene: Research Funding; Takeda: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal